
In 1869, the Australian physician Thomas Ashworth squinted down a microscope and made a curious observation in a blood sample from a metastatic cancer patient: tumor cells.1 Ashworth concluded that shedding tumor cells into the circulation was how primary tumors metastasized to other parts of the body. Decades later, Ashworth’s research findings began to find practical application. Bloodborne tumor cells, it was recognized, could be used to diagnose and monitor cancer. They could even replace tumor tissues obtained by surgical biopsy procedures.
In 1977, scientists discovered an abundance of cell-free DNA (cfDNA) in the blood of cancer patients, especially in metastatic patients, hinting that tumors also shed DNA into the bloodstream.2 That hypothesis was validated in the subsequent decades as advances in sequencing technology allowed scientists to screen for cancer mutations on bloodborne DNA and thereby identify circulating tumor DNA (ctDNA). The ability to interrogate ctDNA—which can be easier to detect than bloodborne tumor cells—opened up a range of new possibilities, from early cancer detection, tracking tumor evolution, and making decisions about therapy selection, all based on a simple blood draw.
Several ctDNA-based “liquid biopsies” have seen U.S. Food and Drug Administration (FDA) approval since 2013, when the agency first gave the green light to a test that quantifies bloodborne tumor cells to predict patient prognosis in certain cancers. In 2016, the FDA approved a ctDNA-based liquid biopsy that detects epidermal growth factor receptor (EGFR) mutations in people with non-small cell lung cancer (NSCLC) to select patients who will benefit from the EGFR-targeting therapy erlotinib. Two comprehensive genomic profiling tests that detect a broad range of mutations, Guardant360 CDx and FoundationOne Liquid CDx, have been approved as companion diagnostics for several therapies that target specific mutations in various cancer types.
“If it seems like the term ‘liquid biopsy’ is becoming as commonplace as ‘precision medicine,’” one scientist wrote in a recent review, “that’s because it probably is.”3
The approvals have encouraged researchers to explore further applications of ctDNA-based liquid biopsies, not only for clinical practice but also for drug development. That was evident at two recent events: the 6th Liquid Biopsy for Precision Oncology Summit, which took place in San Diego in February, and the 12th Annual Clinical & Translational Biomarkers conference, which took place in Boston in June.
Both of these events underscore just how important liquid biopsies have become to drug development. Assays based on ctDNA now help drug developers track the efficacy of drug candidates, select patients for clinical trials, and estimate patients’ risk of disease recurrence. Also, liquid biopsy technology is supporting the development of comprehensive panel tests for a variety of purposes.
Tracking tumor evolution
A Chicago-based diagnostics company called Tempus Labs is developing ctDNA-based profiling tools for clinicians and drug developers. In 2018, it brought to market a liquid biopsy assay, Tempus xF, which screens 105 genes for oncogenic and resistance mutations implicated in a range of solid tumors.
The test is intended to be used together with sequencing of surgical tumor biopsies conducted at diagnosis. According to Nike Beaubier, MD, the company’s senior vice president of life science pathology, cross-referencing ctDNA with tissue DNA allows clinicians to ensure that the observed ctDNA mutations are representative of the tumor genome and don’t stem from unusual cancer cell populations or mutated blood cells present in some people. Then, clinicians can track a tumor’s evolution—including the emergence of resistance mutations—through liquid biopsies.
Beaubier and her colleagues recently tested this approach in a study of metastatic breast cancer patients.4 In addition, as Beaubier noted, the assay can also be used as a standalone tool, for instance, if a “tumor is inaccessible or clinically fragile and you don’t have the opportunity to get tissue.”
One limitation of the 105-gene panel is that it’s not large enough to assess the tumor mutational burden (TMB), a measure of the total number of mutations in a tumor that’s predictive of patient responses to certain immunotherapies, Beaubier said. That’s one reason why Tempus has developed xF+, a more comprehensive panel that screens 523 genes.
Mike Yasiejko, the company’s executive vice president of oncology, said that both panels could aid in drug development “to initially identify what’s happening with a given patient, and then [monitor] longitudinally over time … to understand the evolution of tumor biology.”
Identifying appropriate patients
Meanwhile, the Spain-based biotechnology firm Arjuna Therapeutics is exploring the use of ctDNA-based liquid biopsies to identify patients who are good candidates for its drugs. The company’s lead drug, Ag5, exploits a metabolic vulnerability of cancer cells. Because they typically have a heightened production of damaging molecules called reactive oxygen species (ROS), cancer cells must ramp up on ROS-dampening antioxidants to survive. Ag5 essentially destroys antioxidants, leaving cancer cells with elevated ROS, committing them to cellular suicide.
In a study conducted with scientists from several universities, Arjuna scientists demonstrated that the administration of Ag5 significantly reduced tumor growth in mice with lung cancer. Indeed, tumors became smaller in treated mice and kept growing in untreated control animals.5 “We have some very nice data to suggest that Ag5 will not only work in the primary tumor but also in the metastases,” explained one of the study’s participants, Martin Treder, PhD, chief scientific officer of Arjuna.
Treder noted that although Ag5 targets a process universal across cancer types, certain cancers will likely be more susceptible to Ag5 therapy, perhaps ones with mutations implicated in mitochondrial dysfunction or antioxidant pathways. Liquid biopsies could be used to identify ctDNA mutations associated with a response to Ag5, allowing investigators to select patients most suited for clinical trials. Moreover, the overall presence and quantity of ctDNA—often an indicator of how many cancer cells a patient harbors—could be used to track whether Ag5 is working.
To that end, Arjuna’s scientists are planning to study ctDNA in mouse models with solid tumors treated with Ag5, and to search for mutational signatures that correlate with response. “We’re trying to see what we can detect in the mouse models, and then translate that to the patients,” Treder said.
Monitoring treatment efficacy
Meanwhile, the California-based company Gritstone bio is using ctDNA to track the efficacy of its personalized immunotherapy, Granite. The treatment consists of a series of vaccines designed to provoke T cells into targeting 20 neoantigens identified on the patients’ tumor cells. The vaccine holds particular promise in improving the efficacy of existing immunotherapies in patients with tumors that are resistant to T-cell invasion. Last year, Gritstone reported preliminary data from a Phase I/II study testing the vaccine in combination with checkpoint inhibitor therapies in 26 patients with various kinds of metastatic tumors.6
Throughout the trial, investigators tracked patients’ ctDNA levels through monthly blood draws to assess whether the levels correlate with response to treatment. The assays were designed for each patient, detecting between 50 and several hundred mutations that were identified on tumor biopsies taken prior to treatment.
In a promising sign, the researchers observed an overall drop in ctDNA levels in some patients. Moreover, the drop correlated with the patients’ survival, according to results presented by Gritstone scientists earlier this year: “Five of nine [microsatellite stable colorectal cancer] patients with measurable baseline ctDNA achieved molecular responses … that correlated with [overall survival and progression-free survival], and in some patients, was accompanied by radiologic tumor shrinkage.7
“Cell-free DNA is a real-time measure of potency of the vaccine,” said Karin Jooss, PhD, the company’s head of R&D. The hope is to use ctDNA levels as a preliminary endpoint in clinical studies, and to interrogate why some patients don’t respond to treatment. Jooss emphasized, “This real-time understanding and measure of what the tumor is doing … is very important for real-time managing of patients.”
Integral to clinical development
Kura Oncology, a San Diego-based clinical-stage biopharmaceutical company, is using liquid biopsies across many aspects of its clinical program. That includes using ctDNA as a biomarker to document how tumors change in response to treatment, and to elucidate genetic mechanisms of responses and resistance to treatment.
One of the clinical settings Kura is exploring is NSCLC, where around 70% of patients are ctDNA positive for the EGFR driver mutation at diagnosis and are typically treated with the EGFR-inhibiting therapy osimertinib. Although some 70% of these patients clear their ctDNA within six weeks, around 30% do not. Kura is exploring the use of ctDNA in understanding why these patients have less favorable responses.
The company plans to launch a Phase I study testing whether administering its drug tipifarnib in combination with osimertinib can improve outcomes. The company recently presented preclinical data in mice models of NSCLC suggesting that tipifarnib could prevent relapse to osimertinib for up to six months.8
In the upcoming study, investigators will be closely tracking patients’ ctDNA levels to monitor efficacy. One of the aims of the study is to evaluate whether ctDNA levels can serve as an indicator of treatment efficacy. “We also will be profiling patients all along their longitudinal treatment, looking for those mechanisms of response and resistance,” noted Harris Soifer, PhD, the executive director of clinical biomarkers and companion diagnostics at Kura.
Soifer noted, however, that in certain applications with companion diagnostics, tissue-based analyses are preferred. “Tumor tissue remains the gold standard,” he said. “What’s more, not all patients will have detectable amounts of ctDNA in their bloodstream at the time they are being considered for a clinical trial.”
Tackling minimal residual disease
Other companies, meanwhile, are pursuing an even trickier challenge: developing an assay sensitive and specific enough to detect minimal residual disease (MRD), where trace amounts of ctDNA are present even after intent-to-cure therapy, indicating that a patient still harbors small numbers of tumor cells that could grow back. “This area is a tough challenge because of the very low levels of circulating tumor DNA … in the patient’s bloodstream,” said David Eberhard, MD, PhD, chief medical officer at the Cambridge, U.K.-headquartered Inivata.
Inivata’s InVision liquid biopsy platform overcomes that challenge by employing a highly sensitive sequencing technology called tagged-amplicon deep sequencing (TAm-Seq).9 The assay is designed to screen for up to 48 tumor-specific mutations identified in patients through surgical biopsies, chosen on the basis of how reliably they can be detected through the InVision platform.
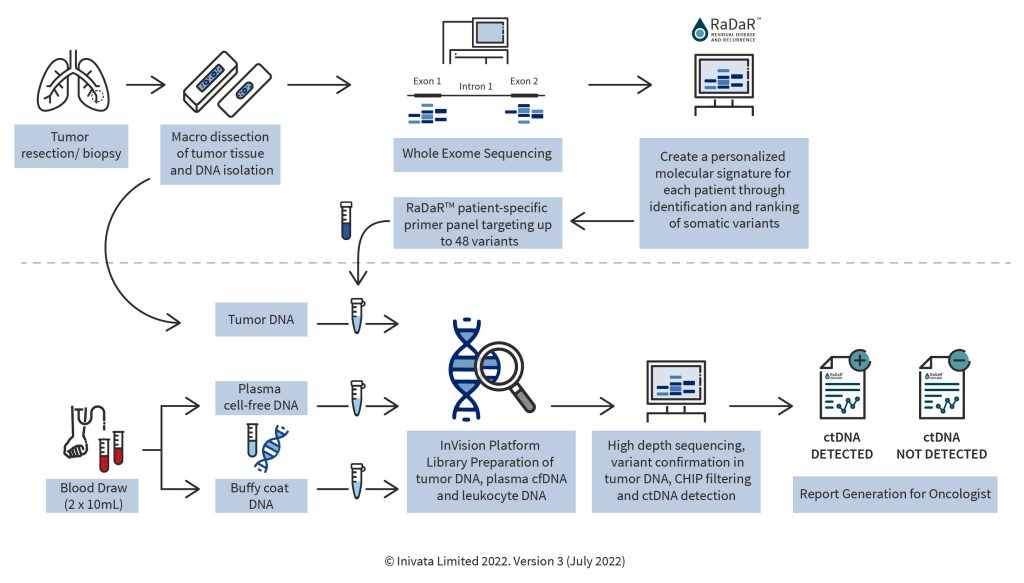
This approach was recently tested in a study of 17 patients with head and neck squamous cell carcinoma.10 ctDNA was detected in all individuals prior to surgery. And in all five patients who experienced a progression, ctDNA was detected at least 108 days before the progression was visible on imaging scans. However, Eberhard added that the ability to detect ctDNA can depend on several factors, including a tumor’s stage, type, and location, which affect how much DNA is shed into the blood.
Nevertheless, he said that the results support the role of ctDNA in estimating a patient’s risk of cancer recurrence, and that they could help inform decisions about therapy selection. The assay could also help in drug development, for instance, by identifying high-risk patients who might particularly benefit from a new treatment. “Throughout the entire patient journey,” he asserted, “it’s easy for us to see where ctDNA could inform patient management decisions.”
References
1. Ashworth TR. A case of cancer in which cells similar to those in the tumours were seen in the blood after death. Aust. Med. J. 1869; 14: 146–147.
2. Leon SA, Shapiro B, Sklaroff DM, et al. Free DNA in the serum of cancer patients and the effect of therapy. Cancer Res. 1977; 37(3): 646–650.
3. Morgan TM. Liquid biopsy: Where did it come from, what is it, and where is it going? Investig. Clin. Urol. 2019; 60(3): 139–141. DOI: 10.4111/icu.2019.60.3.139.
4. Liu MC, MacKay M, Kase M, et al. Longitudinal shifts of solid tumor and liquid biopsy sequencing concordance in metastatic breast cancer. JCO Precis. Oncol. 2022; 6(1): e2100321. DOI: 10.1200/PO.21.00321.
5. Porto V, Buceta D, Domínguez B, et al. Silver clusters of five atoms as highly selective antitumoral agents through irreversible oxidation of thiols. Adv. Funct. Mater. Published March 15, 2022. DOI: 10.1002/adfm.202113028.
6. Gritstone Bio. Gritstone Announces Positive Clinical Data with GRANITE (Individualized Neoantigen Immunotherapy Program) during ESMO 2021 and Launch of Randomized Clinical Trial Program in Colorectal Cancer with Registrational Intent. Published September 17, 2021.
7. Schenk D, Zhou R, Mantilla A, et al. Comprehensive ctDNA monitoring provides early signal of clinical benefit with a novel personalized neoantigen directed immunotherapy for late-stage cancer patients. Poster 4632. Presented at: American Association for Cancer Research Annual Meeting; April 8–13, 2022; New Orleans, LA.
8. Kura Oncology. Kura Oncology Reports Preclinical Data Supporting Use of Tipifarnib to Prevent Emergence of Resistance to Osimertinib in Non-Small Cell Lung Cancer. Published April 8, 2022. https://ir.kuraoncology.com/news-releases/news-release-details/kura-oncology-reports-preclinical-data-supporting-use-tipifarnib.
9. Forshew T, Murtaza M, Parkinson C, et al. Noninvasive identification and monitoring of cancer mutations by targeted deep sequencing of plasma DNA. Sci. Transl. Med. 2012; 4(136). DOI: 10.1126/scitranslmed.3003726.
10. Flach S, Howarth K, Hackinger S, et al. Liquid BIOpsy for MiNimal RESidual DiSease Detection in Head and Neck Squamous Cell Carcinoma (LIONESS)—A personalised circulating tumour DNA analysis in head and neck squamous cell carcinoma. Br. J. Cancer 2022; 126: 1186–1195. DOI: 10.1038/s41416-022-01716-7.