

The promise of CAR T-cell and gene therapies for treating and even curing various medical conditions has the potential to revolutionize countless facets of medicine and its related industries, to say nothing of its effect on human lives and life expectancy. This promise is already well on its way to being fulfilled given the hundreds of trials for cell therapies and other potentially curative treatments currently underway.
The introduction of new curative therapies may seem like a natural advancement in pharmaceutical drug development, but due to the way that these therapies are currently priced (one time high-cost treatments) they are on a crash course with the standard managed-care business model. There are, however, several options being considered to potentially avoid this crash.
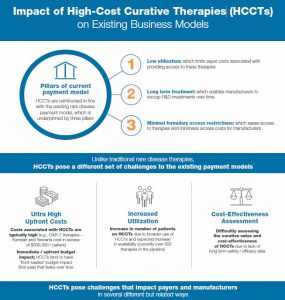
Curative therapies are currently managed and reimbursed in the same way as traditional acute pharmaceutical therapies, but with several important differences. First, the small patient populations and narrow treatment windows lead to a comparatively short time period for manufacturers to maximize their commercial opportunity. In addition, the high clinical benefit associated with a curative therapy means that it could be difficult for payers (the entity paying the manufacturer for the therapy, as opposed to the patient paying to receive it) to manage and triage appropriate patients.
There also can be significant fees associated with hospital procedures and other protocols for administration of gene therapy treatments. And finally, with so many trials underway, the number of treated indications and therapies to be accommodated could expand rapidly. These combined factors could lead to a spike in healthcare costs that could significantly disrupt the U.S. healthcare business model.
Managed care organizations (MCOs) are just beginning to realize the impact that high-cost curative therapies are likely to have on their healthcare delivery business model. With only a few of these products available in the U.S. market today (KYMRIAHTM, YESCARTATM, and LUXTURNATM), the number of patients treated thus far is relatively small. But each therapy comes with a price tag of several hundred thousand dollars, with additional costs for administration. And with new therapies on the horizon, the budget impact is positioned to grow exponentially.
The payers’ view
Charles River Associates recently explored how U.S. payers are likely to interpret the impact of high-cost curative therapies. Interviews with medical and pharmacy directors at major national and regional U.S. payers demonstrated some rapidly emerging concerns:
- Payers broadly expect that high-cost curative therapies will have a substantial first-year budget impact, but that this impact will diminish over time as the “warehouses” of patients are treated.
- Most expect the first-year budget impact to be so high that they need to consider entirely new payment models.
- There is also strong concern that manufacturers will be unable to produce long-term data at launch that is robust enough to evaluate cost-effectiveness over the long term.
Within this environment, payers and manufacturers are considering a range of options in alternative pricing models that can help mitigate the challenges posed by high-cost curative therapies.
Alternative reimbursement models
Among the range of options in alternative pricing models, three have generated some level of support: annuity payments, outcomes-based payment agreements, and commercial- or government-focused risk pools.
Annuity payment models
One of the most popular models under consideration is the annuity payment model. Under this approach, MCOs would make regular payments to therapy manufacturers over a fixed period of time for each patient treated with a curative therapy. For example, payment for a therapy priced at $1 million could be split into 10 base payments of $100,000, with potential considerations for the cost of capital. This payment structure would mitigate the up-front cost and could be gated based on a successful treatment outcome.
While there are clear advantages for this model, it also presents some potentially significant challenges. Payers, for example, might be responsible for continuing payments for patients who have transferred to another insurer, essentially representing a transfer of benefit to a competitor. A second concern is the impact on state budgets, most notably for Medicaid patients where just a few patients treated with these therapies could bankrupt a state’s budget. Finally, there are likely to be government reporting implications (for example, Medicaid best price) and financial reporting issues (such as revenue recognition for the pharmaceutical companies and liabilities for managed care) as a result of an annuity payment model.
Outcomes-based payments
No treatment is guaranteed to succeed for all patients in all cases. An outcomes-based payments model requires that products meet specific clinical targets at predefined time periods to earn reimbursement from payers. If the endpoints are not met, the product is not reimbursed by these payers. In the event treatments fail to achieve these predetermined outcome measures, related costs, such as hospital procedures, would still burden the payer. Outcomes-based agreements help to buffer these costs and also to minimize payer concerns that there is not sufficient evidence at launch to support cost-effectiveness evaluations. Both KYMRIAHTM and LUXTURNATM entered into outcomes-based payments at launch.
All relevant stakeholders will need to align on what constitutes a successful outcome within a predefined time-period. There will be considerable logistical challenges in centralizing outcomes data management and reporting to ensure a consistent flow of high-quality information to relevant stakeholders. Finally, government reporting issues can arise if the failure rate of a treatment falls below the Medicaid best price rate.
Commercial/government risk pools
Many payers are familiar with risk pools including reimbursement models that are either government- or commercially-supported. One active example is the end-stage renal disease (ESRD) program that was established by the U.S. government in the early 1970s to pay for dialysis and kidney transplants. This program allows for many individuals with ESRD to receive Medicare benefits regardless of their age. A similar program could be set up for many conditions that can be treated with high-cost curative therapies in the years ahead. This would allow commercial payers to carve out their risk of patients receiving these therapies for a limited period of time, which would help to keep premiums and cost sharing at more reasonable levels.
Many payers note that expansion of government-sponsored risk pools may be unlikely in the current political climate. They also anticipate challenges in achieving the necessary levels of broad alignment among U.S. payers to engage in this type of endeavor commercially. The cost of this payment model may also be difficult to estimate based on the small number of approved products and the lack of efficacy data across all next-generation curative therapies.
Conclusion
We have yet to find the silver bullet that can reward manufacturer innovation while simultaneously proving cost effective for payers. While U.S. payers are concerned about the budget ramifications of curative therapies and do not believe that increases in premiums and patient cost sharing can continue to sustainably support the new pricing models needed for high up-front cost of care, they are far from aligned on the appropriate actions to take to mitigate rapidly rising therapy and administration costs.
Solutions could involve a combination of elements of the models outlined above. It also seems likely that a solution will require some explicit acknowledgement by the government of this challenge to keep price-reporting/best-price calculations from limiting payment innovations. The accelerating pace of progress in clinical development means that time will soon become a critical issue as more and more of these therapies emerge from clinical research and are positioned to deliver significant benefits to patients who can access them.
Matthew Majewski is a vice president in Charles River Associates’ life sciences practice. The views expressed herein are the author’s and not those of Charles River Associates or any of the organizations with which the author is affiliated.
