
John Sterling Editor in Chief Genetic Engineering & Biotechnology News
If Not Tackled Now, by 2050, the Death Toll Could Be One Person Every Three Seconds
Microbial drug resistance (MDR) is a huge, worldwide health problem due to the overprescribing of antibiotics. What’s worse: there are no signs that things are going to get better anytime soon, with most of the indirect impact of MDR affecting developing countries.
The U.K. government, with support from the Wellcome Trust, recently published a review on MDR to address this serious issue. Entitled “Tackling drug-resistant infections globally: Final report and recommendations for the growing global problem of drug-resistant infections,” the study estimates that by 2050, 10 million lives a year and a cumulative $100 trillion of economic output are at risk due to the rise of drug-resistant infections, if solutions are not found to slow down the rise of drug resistance. Currently, 700,000 people die of resistant infections every year.
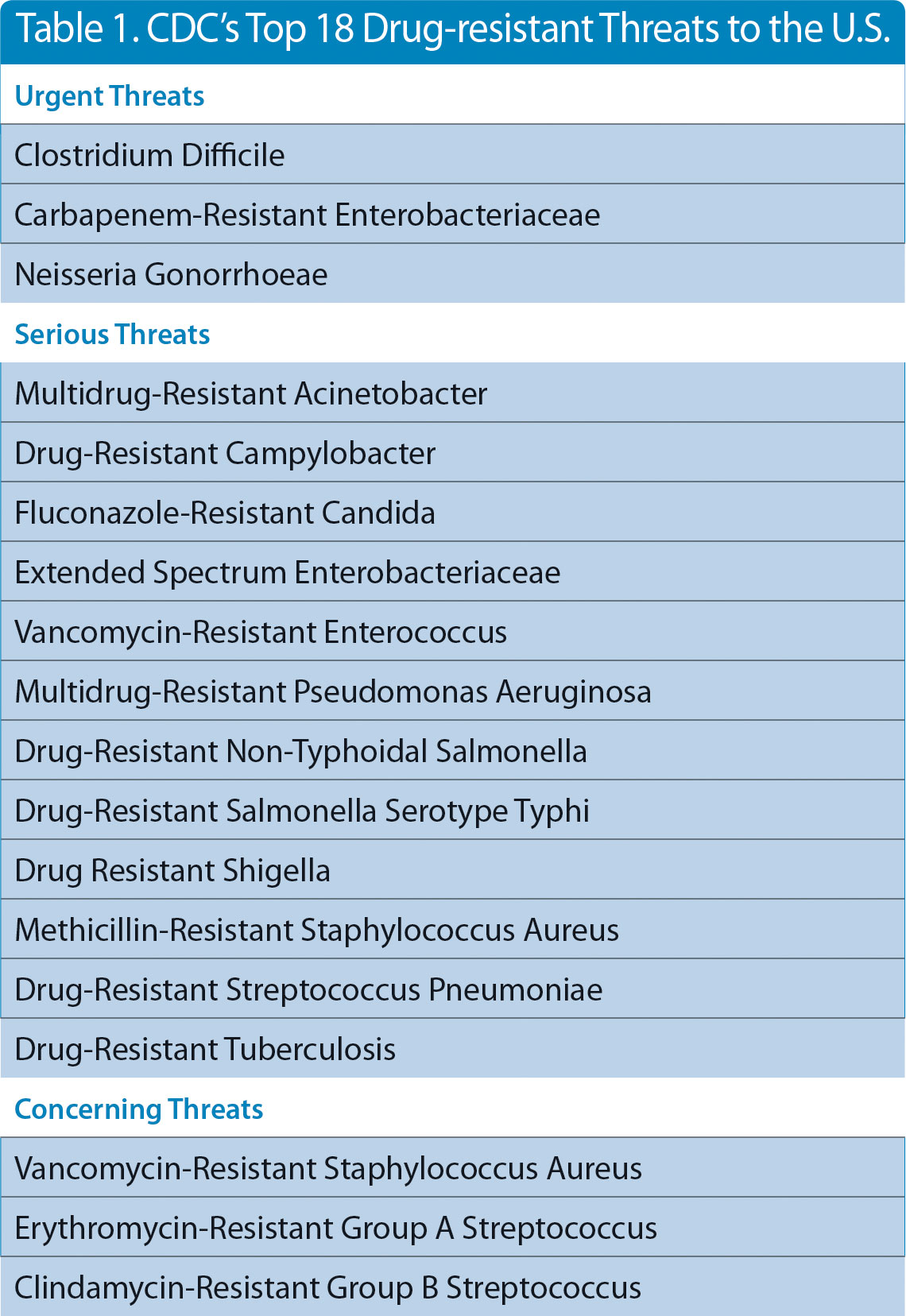
Four years ago, the CDC published a list outlining the top 18 drug-resistant threats (Table 1) to the U.S. Last fall, to further illustrate the growing concern over MDR, the U.S. government launched a prize competition calling for innovative ideas for rapid, point-of-care laboratory diagnostic tests to combat the spread of drug-resistant bacteria. Antibiotic-resistant bacteria cause at least two million infections and 23,000 deaths each year in the U.S., according to the CDC.
The Antimicrobial Resistance Diagnostic Challenge, sponsored by the NIH and the Health and Human Services Office of the Assistant Secretary for Preparedness and Response, will award $20 million in prizes over all phases of the competition for new lab diagnostics, specifically those that identify and characterize antibiotic-resistant bacteria and those that distinguish between viral and bacterial infections to reduce unnecessary uses of antibiotics, a major cause of drug resistance.
GEN recently interviewed several company officials focusing on developing new diagnostics and treatments for MDR. Most of the companies GEN interviewed are working on therapeutics to deal with MDR; although one firm, OpGen, is diagnostics centered.
OpGen
Evan Jones, a long-time bioindustry veteran, currently serves as chairman and CEO of OpGen. He agrees that the MDR problem is growing and is most common in acute care settings and more centralized in big cities in the U.S.
“We did a large outcomes study with Intermountain Health in Utah. We looked at three or four million health records of patients suffering from drug-resistant infections,” Jones told GEN. “High on the list are people with co-morbidities, an acute care patient with diabetes or pulmonary disease, or cancer patients. But the hotbed in the U.S. is long-term care facilities, due to the high use of antibiotics.”
He points out that developing countries such as India, Turkey, and Greece and regions including Southeast Asia and Eastern Europe have the most significant difficulties in dealing with MDR.
Jones says he became interested in the diagnostic opportunity, thinking in terms of genomics and informatics, five years ago, when the CDC started putting out guidance documents saying that they needed to screen people for drug-resistant pathogens.
“At the time, the CDC suggested that people get screened with culture methods and I thought that this area was ripe for industrialization with genetic technology,” he points out. “So that is where we began, but we have moved to a more general view of using this information to develop rapid DNA tests to guide antibiotic decision-making, the rapid one-hour tests that can tell you what drug to get.”
OpGen is zeroing in on MDR genes. The company has a relationship with Merck Pharma to look at its global monitoring database, which includes about 175 hospitals worldwide and hundreds of thousands of microbes.
“We are picking the representative bugs from all over the world. We have a genomics pipeline that both sequences and also does production genomics, so more high-throughput, and marries the results with the phenotypic information for antibiotic susceptibility and puts that together into what we call the Lighthouse Knowledge Base,” explains Jones, adding that Knowledge Base can derive predictive information. With that predictive information, three businesses can be powered: rapid diagnostics, hospital efficiency, and Pharma decision-making.
The pathogens OpGen works with range from viruses to Gram-positives (e.g., staph infection), to fungi, to Gram-negatives. The Gram-negatives are probably the most complex from the genomic resistance perspective, and that is where we are focused, says Jones.
“Right now, we are taking those genes that we have picked and are making rapid diagnostic kits,” he notes. “We expect the first ones to be available for research use later this year.”
Entasis Therapeutics
Although not a diagnostics company, Entasis Therapeutics is using genomics internally for its drug discovery efforts.
“We are using genomic methods to modify bacteria to study their mechanisms of antibiotic uptake, so we can develop cellular systems that let us try to have a deeper understanding of what is going on when a molecule interacts with a bug, how the bug reacts in terms of allowing it in, what the structural features are required of molecules to get into bacteria better, and what makes bacteria spit them out, efflux them more effectively,” points out Ruben Tommasi, Ph.D., CSO at the company. “Our goal is to combine those efforts with potent compounds on targets that we know work, so that we can design better antibiotics.”
In the opinion of Manos Perros, Ph.D., CEO, the use of those genomic tools makes Entasis different from other companies developing drugs to combat MDR.
“Antibiotics traditionally were discovered empirically. You would screen a large collection of molecules against a living bug and see which ones worked. If they worked, great. You then develop them as an antibiotic.”
Echoing Dr. Tommasi, Dr. Perros explains that Entasis works on understanding how bacteria get killed by those drugs and how those drugs penetrate the second shell of a microbe. The company then applies science to design molecules that kill the microbe effectively.
“Another approach has been to take a molecular target, a protein, and find active molecules against that,” continues Dr. Perros. “Both approaches have limitations. Both have had successes. But in the last decade, neither has actually delivered a new class or a clearly differentiated antibiotic.”
Entasis’ approach is an example of science at work, according to Dr. Perros, who adds that the company has a discovery group that does this work under Dr. Tommasi’s leadership. “The results are molecules like the ones that we have now in the clinic against highly resistant pathogenic bacteria,” he says.
As for the investigational drugs that the company is currently studying in the clinic, they are zoliflodacin, the first in a novel class of topoisomerase inhibitors which successfully completed Phase II clinical trials against gonorrhea in 2016 (the study was conducted by the NIH); and ETX2514, a broad-spectrum beta-lactamase inhibitor that the firm is initially developing in combination with sulbactam against infections caused by Acinetobacter baumannii (currently in Phase I).
Auspherix
Auspherix is an anti-infectives company engaged in the discovery and development of a new class of organogold-based antibiotics for serious, difficult to treat, or potentially life-threatening infections. Its new class of antibiotics demonstrate potent and broad-spectrum activity against both Gram-positive and Gram-negative bacteria, including many Gram-negative multidrug resistant strains where there is a global rising unmet medical need and large market potential, according to Neil Miller, Ph.D., CEO., who favors the traditional phenotypic screening approach to new drug discovery to combat MDR bacteria.
Dr. Miller says that bacterial genomics has improved our understanding of infection in several ways: The application of genomic epidemiology to outbreaks of disease (e.g., in a hospital environment) has increased our ability to diagnose not only the organisms likely responsible for disease, but also identify the antibiotic resistance determinants carried by that organism. “It is hoped this approach will ultimately result in improved diagnosis, as well as increase the success of treatment regimens,” he tells GEN.
The “essential gene” argument has been used to define the entire repertoire of genes in a target organism that are required for survival and growth, explains Dr. Miller. As these gene products are essential for bacterial viability, expression of the cognate proteins followed by screening against libraries of small molecules has been a popular approach used to attempt to find novel antibacterial drugs.
“Unfortunately, this approach has not been very successful and drug discovery has now moved on to alternative approaches where genome information can be used to help identify the mode of action [MOA] of a drug candidate following its identification,” notes Dr. Miller.
Following the failure of the essential gene approaches in the late 1990s–early 2000s, Auspherix’s founders embarked on a target-agnostic phenotypic screening strategy—a strategy that was employed historically during the golden era of antibiotic discovery. By screening against a library of FDA-approved medicines they ensured that any hit molecules came from known a drug-like chemical space; thus, there was a higher likelihood of successfully progressing through the various phases of drug development, he remarks.
“This approach identified auranofin (Ridaura), a medicine marketed for arthritis in the 1980s which belongs to a small class of organogold drugs (i.e., containing a gold atom) that have a long history of clinical use in man,” Dr. Miller says. “Although encouraged by its potent activity against S. aureus (a Gram-positive bacteria) in different growth states (planktonic, biofilms and persister cells), auranofin had minimal activity against Gram-negative bacteria for which the greatest unmet medical need exists.”
The team at Auspherix, has gone on to discover three chemical series of organogold compounds that have “potent” broad-spectrum activity against both Gram-positive and Gram-negative bacteria, says Dr. Miller, including the so-called ESKAPE (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter, Pseudomonas aeruginosa, and Enterobacter) pathogens or superbugs which cause the majority of serious hospital infections.
Importantly, Auspherix’s compounds retain activity against multi-drug-resistant strains of these bacteria and initial data suggest that there is a low propensity for the emergence of resistance to the Auspherix compounds, clearly a highly desirable property for any new antibiotic, according to Dr. Miller.
“It is believed likely that auranofin and the Auspherix compounds do not act via a single molecular target and that a more complex mode of action is involved which consequently limits the ability of bacteria to develop resistance,” he says. “The Auspherix compounds show antibacterial activity following intravenous or oral dosing in rodents and are now being tested in vivo in models of bacterial infection.”
Auspherix was founded in late 2013 and is currently engaged in preclinical R&D only. Its lead drug-discovery project is in the lead optimization phase, and the company expects to progress into clinical trials in early 2019.
“We are targeting complicated urinary tract infections (cUTI) as a lead indication, but are also exploring the potential to expand into additional indications such as hospital-acquired bacterial pneumonia (HABP) or complicated intra-abdominal infections (cIAI),” notes Dr. Miller. “If successful, it is anticipated that a new medicine from Auspherix’s novel class of organogold antibiotics may reach the market around 2025.”

