
The riches of gene therapy now include Casgevy, the recently approved ex vivo gene editing therapy. Many other riches await, and some of them are quite different from those within reach of traditional or ex vivo gene editing approaches. For example, riches are emerging that are unique to in vivo gene editing, which involves the intravenous or local delivery of gene editing tools directly to patients.
Ultimately, gene editing tools must enter patients’ cells. There are two main forms of cell delivery: viral and synthetic (nonviral). Both are in use in clinical trials evaluating in vivo gene editing therapies for hereditary disorders and acquired diseases including atherosclerotic arterial and infectious diseases.
Editing on the beam

Chief Medical Officer, Beam Therapeutics
In vivo gene therapies can be delivered via a nonviral vehicle known as the lipid nanoparticle (LNP). It is well known to Amy Simon, MD, the chief medical officer at Beam Therapeutics. Before joining Beam three years ago, Simon was responsible for developing RNA interference therapies at Alnylam. For example, she was the lead clinician developing Givlaari (givosiran), an RNA interference therapy for patients with acute hepatic porphyria. Givlaari, which was approved by the FDA in 2019, is delivered via an LNP.
At Beam, Simon faced familiar uncertainties concerning LNP delivery. “We didn’t know if this would work in people,” Simon recalls. “Even although you could argue that LNPs in vivo have been very de-risked since [my early days] at Alnylam, it was like, ‘How do you even get there?’”
Regardless of the LNP challenges, Simon wants to make sure that the Beam pipeline has as many “shots on goal” as possible. For example, in Beam’s development of therapies for hemoglobinopathies, she is helping the company prioritize the ex vivo approach because it seems to be the easiest way to successfully deliver gene editing tools.
Simon points out that Beam sees three waves of innovation that will progressively expand the reach of its ex vivo approach to broader subsets of patients. In the first wave, cells modified via base editing are delivered in an autologous bone marrow transplant after genotoxic conditioning. In the second wave, genotoxic conditioning is avoided through the use of an alternative conditioning platform, which Beam calls Engineered Stem Cell Antibody Paired Evasion. In the third wave, which Simon calls the “holy grail,” gene editing tools are delivered to patients through intravenous infusion of LNPs targeted to hematopoietic stem cells (HSCs), eliminating the need for transplantation altogether.
Beam also has plans beyond developing treatments for hemoglobinopathies. The company is using in vivo gene editing to pursue treatments for alpha-1 antitrypsin deficiency and Stargardt disease. In the former treatments, LNPs are being used to target the liver; in the latter treatments, adeno-associated viral vectors are being used to target the eye.
“People don’t like using the phrase plug-and-play, but at least you start to develop competencies that you can now kind of utilize,” Simon observes. “It becomes a little more platform-like, where you can even start to use different products and programs to support your other programs. Your regulatory filings get a little bit better because you’re using your top studies from that same product as support.”
One example of a platform-like competency is optimized editor technology—in Beam’s case, base editor technology. A base editor can be paired with different single guide RNAs for flexibility in targeting DNA (and addressing different indications), and with different LNPs for flexibility in delivering the gene editing tools to different kinds of cells. Indeed, base editor competency can even facilitate the transition from ex vivo to in vivo gene editing. For example, the same editor and guide from an ex vivo application can be combined with a vector suitable for in vivo delivery, avoiding transplantation altogether.
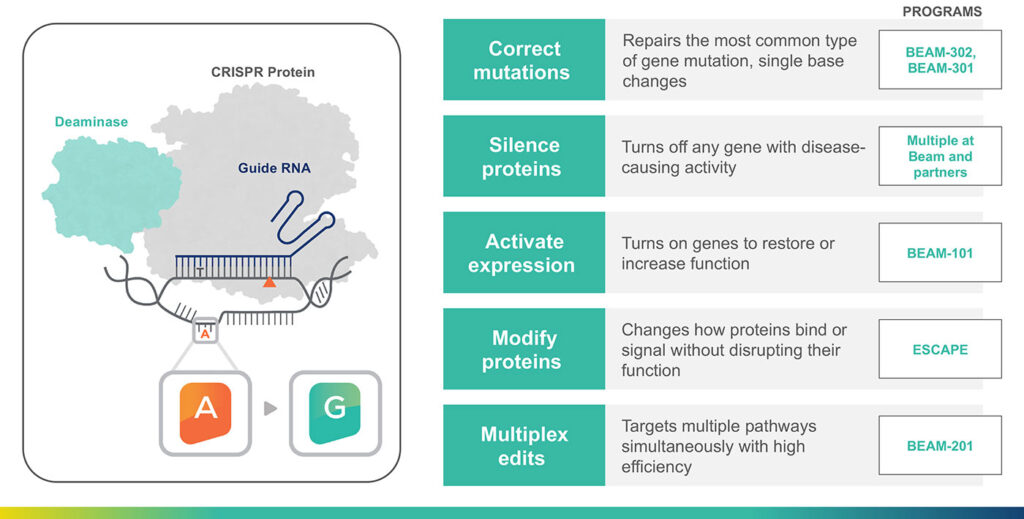
“Patients had nothing new for years, since the 1980s,” Simon notes. “But now we hear lots of excitement about the fact that there’s finally CRISPR-based approval for sickle cell disease.” She goes on to suggest that more excitement is coming, thanks to the development of CRISPR technology that avoids double-strand breaks that can result in unwanted chromosomal abnormalities and genotoxic stress. One such CRISPR technology is Beam’s base editor, which Simon calls a “kinder and gentler CRISPR.”
To support her assertion, Simon cites preclinical data indicating that BEAM-101 features high levels of HSC editing (over 90% of alleles edited), high and consistent levels of upregulation of fetal hemoglobin (over 60% of total hemoglobin), and significantly lower levels of sickle cell hemoglobin (less than 40% of total hemoglobin). Ultimately, the levels of fetal and of sickle cell hemoglobin are similar to those of sickle cell trait carriers who do not have sickle cell disease.
Incorporating base editors in a platform approach has enabled Beam to advance several programs. For example, the BEAM-101 program for sickle cell disease is entering the clinic and expected to yield data by the end of the year. Also, Beam is starting an alpha-1 antitrypsin deficiency study. The company hopes to dose the first patient in this study during the first half of 2024.
“We’ll have data really starting to show what base editing can do,” Simon predicts. At Beam, the hope is that base editing will result in healthier cells and enable the development of highly differentiated programs.
Ready for prime time
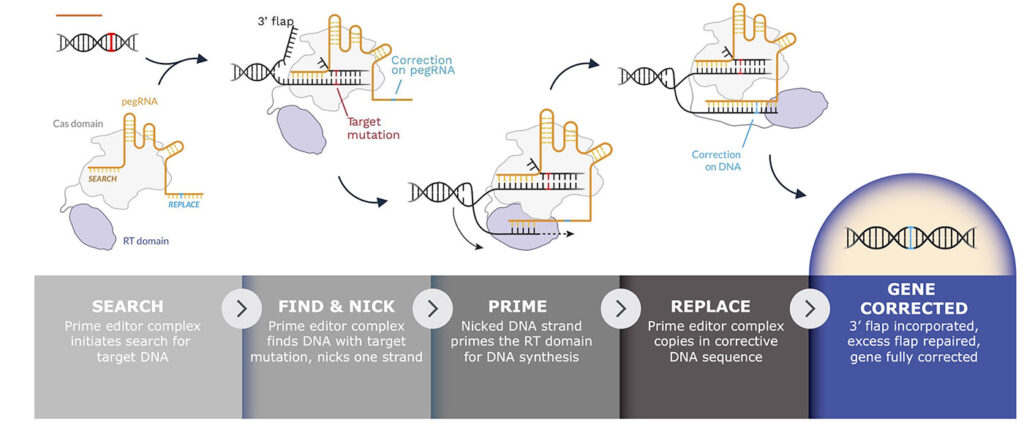
Similarly to Beam Therapeutics, Prime Medicine emphasizes one kind of CRISPR editor. At Prime, that editor is, well, a prime editor. Prime Medicine has several programs that span ex vivo to in vivo, and the company is planning on filing an IND and/or CTA with various countries by the first half of this year with the goal of delivering clinical data by 2025.

Senior VP, Prime Medicine
“Prime editing has the unique ability to address these rare genetic diseases for which there are no available treatments,” says Mohammed Asmal, MD, PhD, senior vice president and head of clinical at Prime Medicine. “Initially, we tried to focus on diseases that are associated with high unmet needs and that present good targets for prime editing.” The best targets are mutations for which prime editing is the most effective technology available.
The first program that Prime Medicine is bringing to the clinic is for a rare immunodeficiency called chronic granulomatous disease. Prime’s approach to treating this brain deficiency is an ex vivo autologous HSC transplant, a modality that’s been extensively de-risked for gene therapy. This approach is particularly well suited to treating P47phox-deficient chronic granulomatous disease, which is caused by a dinucleotide mutation that is amenable to correction by prime editing. Prime has already demonstrated very efficient editing of this locus in mouse models.
Parallel to this, Prime Medicine has entered into a collaboration with Cimeio Therapeutics to improve the safety and effectiveness of HSC transplants for genetic diseases, acute myeloid leukemia, and myelodysplastic syndrome. Cimeio is developing a shielding mechanism that allows HSCs to be protected from antibodies without losing their native functionality.
“[Cimeio’s technology] is reliant on prime editing to enable the introduction of the exquisite mutations that are required to confer resistance to an antibody on a surface receptor while preserving the function of that receptor,” Asmal explains. “Prime editing can give the shielding, and this allows, we hope, the future of HSC transplantation to be free of myeloblative conditioning. So, you can essentially put this edit into HSCs, and then you can use an antibody to deplete the unshielded HSCs and get your gene edited HSCs to take over.”
The next set of in vivo programs closest to the clinic are for indications in the liver, such as glycogen storage disease 1B (GSD1b) and Wilson’s disease, and for indications in the eye, such as retinitis pigmentosa.
“Initially, the idea was to go broadly and establish that we can do this in multiple different tissue types,” Asmal relates. “[This approach resulted in a] pipeline that covers everything from the HSC space to the eye, the liver, and the neuromuscular system.
“Several of the targets we pursue have much more validated mechanisms of delivery. For example, the delivery challenges for HSCs are much more tractable than those for the neural system. As we make progress in delivery, we may see more clearly where we should go and where we should focus our efforts.”
Going viral
Whereas Beam Therapeutics and Prime Medicine are going after genetic diseases that affect relatively small patient populations, Excision Bio is going after infectious diseases that affect populations of patients in the hundreds of millions. In a sense, Excision Bio is focusing on the other end of the spectrum of human health and disease.

Chief Executive Officer, Excision Bio
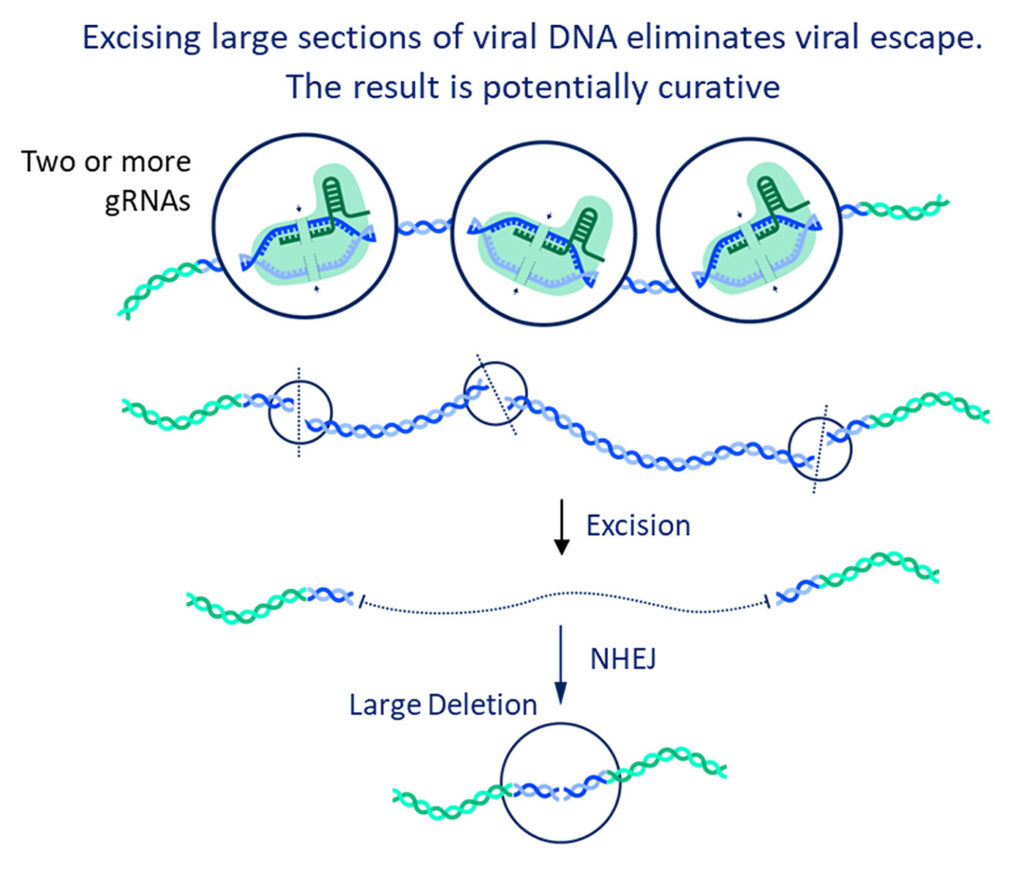
“We target viral DNA,” says Daniel Dornbusch, Excision Bio’s CEO. “The big difference between Excision Bio and the others in the [gene editing] space is that we’re looking only at nonhuman DNA to cut and remove.
“In a lot of ways, we are using CRISPR the way it evolved in nature, which is to defend against viruses. We’re using CRISPR to target human DNA instead of bacteriophage DNA, but it’s really the same concept. We’re eliminating nonnative DNA. We’re not trying to add or correct something. We are just trying to return the body to a normal state by removing something that shouldn’t be there in the first place.”
Excision Bio doesn’t attempt to get at a virus while it’s infecting an individual. Acting within such a narrow window would be difficult even if an effective means of countering infection were readily available. Instead, Excision Bio has a strategy of treating people who have already contracted infectious diseases such as HIV disease or hepatitis B. The existing therapies are antivirals that reduce the level of replication, but none of them go to the source of the infection. None remove the viral DNA the virus
has put into human genomes.
To excise viral DNA, Excision Bio has built a bioinformatics platform that integrates computational methods to design the most effective guide RNAs, and that leverages in silico design to generate probes for analyzing on- and off-target effects. The hard part of Excision Bio’s work isn’t identifying which DNA regions need to be removed. Instead, it’s figuring out what will happen to the human DNA after the viral DNA is cut out. Uncertainties include the specificity of excision across patients, and the quality of DNA repair at the target site.
Excision Bio has developed EBT-101, an investigational gene therapy for HIV-1. Its components, which include a dual-guide CRISPR-Cas9/gRNA multiplex and an adeno-associated viral vector, are designed to enable targeting of latent HIV-1. The therapy was shown to remove large sections of HIV proviral DNA in humanized mice and nonhuman primates, and it is now being evaluated in an open-label, multicenter, Phase I/II trial. The trial dosed its first patient in September 2022 and was granted fast track designation by the FDA in July 2023.
“We’ve not detected off-target editing, structural variations, or adeno-associated virus insertions in mice, humans, or nonhuman primates above the error rates of assays, we believe, because our guide sequences are so different from natural human sequences,” Dornbusch reports. “Thus far in the clinical trial, we have seen only grade-one side effects related to the drug, and these resolved on their own.”
The company will be presenting additional clinical trial data in May, at this year’s meeting of American Society of Gene and Cell Therapy. “What is the safety of CRISPR when delivered systemically?” Dornbusch asks. “Our data combined with data from an Intellia Therapeutics trial seems to answer that question. So far, the safety looks good, which should clear the way for additional trials, indications, and modalities.”
